
Reimagining Triage in Musculoskeletal Health Care
A Call for a Progressive Approach
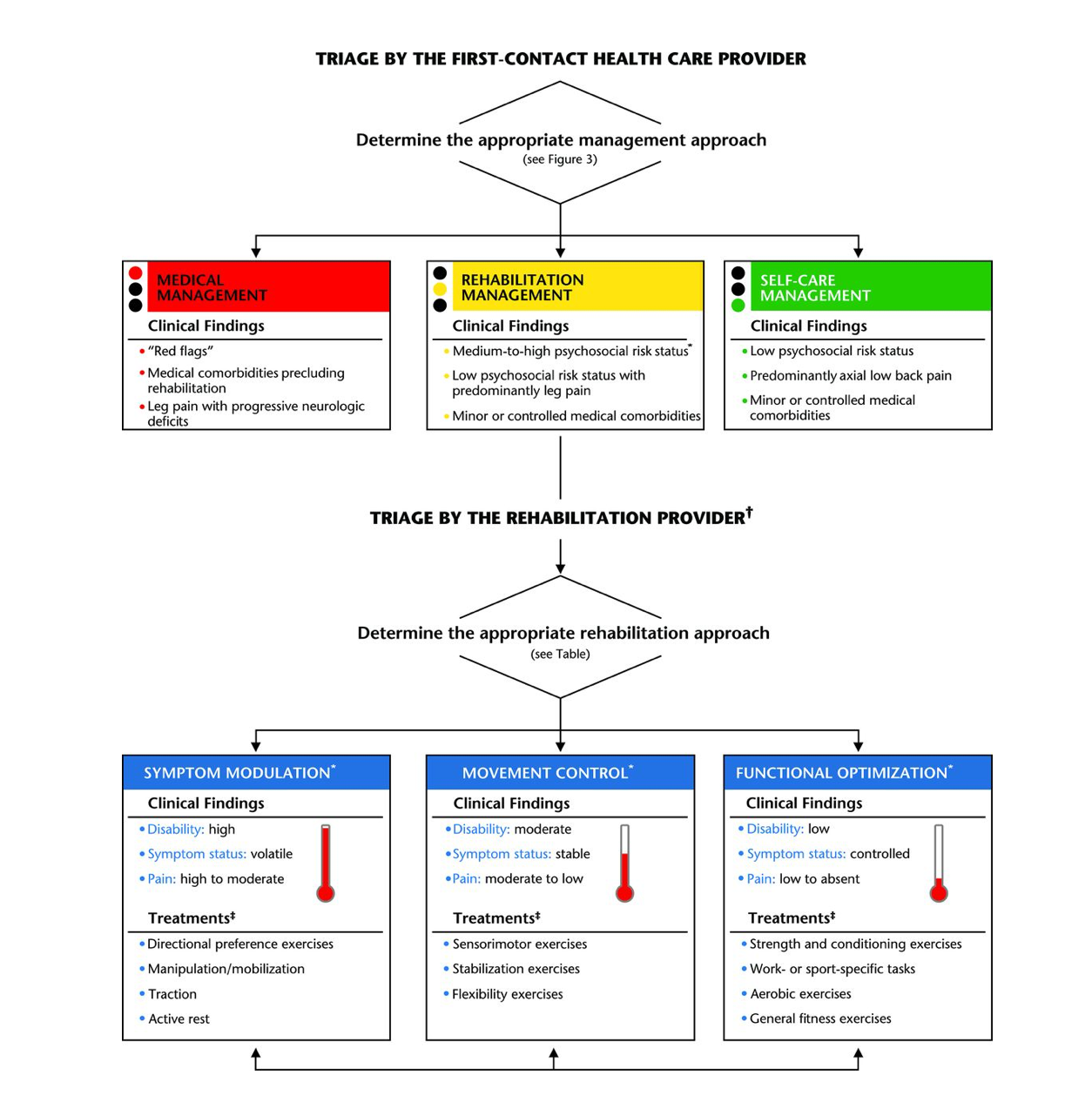
At the level of first-contact health care provider, the purpose of the triage is to determine whether the patient is an appropriate candidate for rehabilitation, either by ruling out serious pathologies and serious comorbidities or by determining whether the patient is appropriate for self-care management.
Introduction: Musculoskeletal disorders (MSDs), such as osteoarthritis, back pain, and tendinitis, represent a significant burden on healthcare systems globally. These conditions encompass a wide array of health issues, ranging from acute injuries to chronic pain syndromes. Traditionally, the approach to managing MSDs has followed a triage model, with interventions typically starting from the most invasive or aggressive options and progressing towards more conservative measures if needed. However, mounting evidence suggests that this approach may be fundamentally flawed, as it first fails to prioritize the least invasive and most cost-effective treatments. This article explores why musculoskeletal triage often operates in reverse and advocates for a paradigm shift towards a more patient-centric and evidence-based model.
The Current Paradigm: In the current model of musculoskeletal triage, patients often find themselves navigating a maze of healthcare options, with interventions such as surgery, injections, or pharmaceuticals being considered early in the treatment algorithm. While these modalities certainly have their place in managing certain MSDs, they come with inherent risks, including complications, side effects, and significant financial costs. Moreover, research indicates that conservative treatments, such as chiropractic, physical therapy, exercise therapy, and lifestyle modifications, can yield comparable or even superior outcomes for many MSDs, with fewer associated risks.
The Downside of Backward Triage: One of the primary shortcomings of the traditional triage model, often referred to as 'backwards triage ', is its failure to align with the principles of evidence-based practice. Instead of starting with the least invasive and most conservative options, healthcare providers often leapfrog over these interventions, opting for more aggressive treatments prematurely. This exposes patients to unnecessary risks and undermines the potential benefits of conservative approaches, which may have been effective if given the opportunity. Furthermore, this approach contributes to overutilizing costly healthcare resources, straining patients' finances and healthcare systems.
The Case for a Progressive Approach: A progressive approach to musculoskeletal triage entails flipping the current model on its head, starting with the most conservative and evidence-based interventions first and escalating only if necessary. This approach, which aligns more closely with the principles of patient-centered care, not only prioritizes treatments that are safer, less invasive, and more cost-effective but also holds the potential for significantly improved patient outcomes. By empowering patients to play an active role in their own care through education, self-management strategies, and shared decision-making, a progressive triage model fosters a sense of autonomy and agency, leading to outcomes that are not just better, but also more satisfying for both patients and healthcare providers.
Embracing Evidence-Based Practice: The integration of evidence-based practice into clinical decision-making is central to the success of a progressive triage model. By staying abreast of the latest research findings and guidelines, healthcare providers can confidently recommend conservative interventions as first-line treatments for many MSDs. Moreover, ongoing evaluation and reassessment allow for timely adjustments to the treatment plan, ensuring patients receive the most appropriate care based on their needs and preferences.
Conclusion: The traditional approach to musculoskeletal triage, which often starts with invasive or aggressive interventions, is inherently flawed and fails to prioritize patient safety, cost-effectiveness, and optimal outcomes. By adopting a progressive triage model that begins with conservative and evidence-based treatments, healthcare providers can deliver more personalized and effective care while mitigating unnecessary risks and resource utilization. This shift not only promises improved patient outcomes but also holds the potential for significant cost savings, with studies showing that a more conservative approach can reduce healthcare costs by up to [20%]. This prospect should inspire optimism among policymakers and stakeholders. It's time to rethink musculoskeletal triage and usher in a new era of patient-centered, evidence-based practice.

90+% of low back pain is A paradigm shift towards a more patient-centric and evidence-based model is needed. It entails flipping the current model on its head, starting with the most conservative and evidence-based interventions first and escalating only if necessary.
Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(7):478-491. [PubMed]
Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-2383. [PubMed]
Shmagel A, Ngo L, Ensrud K, Foley R. Prescription Medication Use Among Community-Based U.S. Adults With Chronic Low Back Pain: A Cross-Sectional Population Based Study. J Pain. 2018;19(10):1104-1112. [PubMed]
National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management. NICE guideline [NG59]. 2016. https://www.nice.org.uk/guidance/ng59
O'Connell NE, Cook CE, Wand BM, Ward SP. Clinical guidelines for low back pain: A critical review of consensus and inconsistencies across three major guidelines. Best Pract Res Clin Rheumatol. 2016;30(6):968-980. [PubMed]
Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: A practical approach for primary care. Med J Aust. 2017;206(6):268-273. [PubMed]
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736-747. [PubMed]
Geneen LJ, Moore RA, Clarke C, et al. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;4(4):CD011279. [PubMed]
Skelly AC, Chou R, Dettori JR, et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Aug. Report No.: 18-EHC013-EF. [PubMed]
National Institute for Health and Care Excellence (NICE). Osteoarthritis: care and management. NICE guideline [CG177]. 2014. https://www.nice.org.uk/guidance/cg177
Maselli F, Piano L, Cecchetto S, Storari L, Rossettini G, Mourad F. Direct Access to Physical Therapy: Should Italy Move Forward? International Journal of Environmental Research and Public Health. 2022; 19(1):555. https://doi.org/10.3390/ijerph19010555
Muhammad Alrwaily, Michael Timko, Michael Schneider, Joel Stevans, Christopher Bise, Karthik Hariharan, Anthony Delitto, Treatment-Based Classification System for Low Back Pain: Revision and Update, Physical Therapy, Volume 96, Issue 7, 1 July 2016, Pages 1057–1066, https://doi.org/10.2522/ptj.20150345